Unfortunately, ear canal opening surgery is abused by some surgeons around the world. We know of hundreds of patients who have been deceived by the promise of results that will never happen and whose lives have been ruined by terrible complications arising from canal surgery. These patients experience a great disappointment instead of an increase in hearing. In order to get rid of the infection and smelly discharge in the opened canal, it is necessary to close the canal and they have been operated on many times for this.
TO WHOM CAN IT BE DONE?
Children with unilateral microtia can lead a normal life like their peers without needing any hearing aid, while those with bilateral microtia can lead a normal life like their peers with the support of a hearing aid. The only problem they will experience is related to the direction of sound in noisy environments, and they adapt to this situation over time.
For patients with unilateral microtia, who can lead an extremely normal life without using a hearing aid, there is no need to open the auditory canal at all. However, in patients with bilateral microtia and with a score of 7 and above in the middle ear assessment with high-resolution CT, ear canal opening can be tried to improve hearing. Otherwise, it is a rather risky and not beneficial operation. In order to decide the issue, the findings detected by CT (COMPUTERIZED TOMOGRAPHY) after the age of 5 should be evaluated according to the JAHRDORSFER classification. It is not recommended to do this earlier, since during the tomography examination your child will receive a high dose of radiation.
HDCT
High Definition
Computerized Tomography
This examination is performed to evaluate the ear canal and middle ear structures. Tomography findings are evaluated with the "JAHRSDOERFER CLASSIFICATION" and a score between 0-10 is determined. This score is decisive in deciding whether to open the ear canal in a child with microtia. According to this scoring, at least 7 points are required to decide on a channel opening attempt. In other words, channel opening should not be attempted in cases with a score lower than 7.
WILL MY CHILD HEAR BETTER IF THE EAR CANAL IS OPENED?
This examination is performed to evaluate the structures of the auditory canal and middle ear. Tomography findings are evaluated with the "JAHRSDOERFER CLASSIFICATION" and a score between 0-10 is determined. This score is indicative in deciding whether the auditory canal should be opened in a child with microtia. According to this scoring, at least 7 points are required to make a decision on an attempt to open a canal. In other words, canal opening should not be attempted in cases with a score lower than 7.
THE RISKS OF OPENING THE CANAL
FACIAL PALCY
DAMAGE TO THE AUDITORY NERVE
(PERMANENT HEARING LOSS, TINNITUS, VERTIGO etc.)
CHRONIC INFECTION - EAR DISCHARGE
Painful cleaning attempts every 2-3 months, patients who cannot go into the pool or sea for a lifetime
NARROWING THE CANAL BY TIME
OBSTRUCTION
Separation of the "eardrum" (requires surgery to correct it)
THE HEARING INCREASE AT THE EARLY STAGE IS GRADUALLY REDUCED DUE TO COMPLICATIONS
The surgery for opening the canal is usually requested by parents who do not do search on the subject, but as they investigate the subject, their desire for the surgery disappears due to serious risks.
MYTHS & FACTS ABOUT CANAL SURGERY
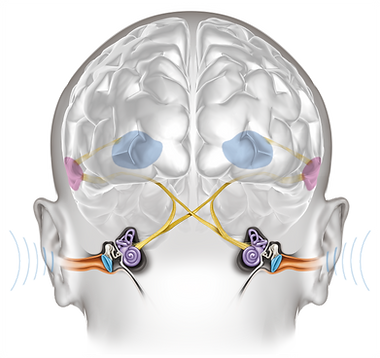
IF YOU DO NOT OPEN THE CANAL YOUR CHILDS BRAIN WILL NOT DEVELOP!
WRONG ! The auditory system, unlike the visual system, sends signals from both ears to both sides of the brain. The central auditory pathways cross the midline very early in the auditory pathway, so that both sides of the brain receive stimulation from both ears. This means that in cases of unilateral microtia, both sides of the brain are stimulated by the well-hearing ear. The argument that the sooner the surgeon opens the atretic ear, the less chance the brain will "turn itself off" (and not being able to respond) to the inputs from the reconstructed ear is completely false and misleading. Patients, whether they undergo atresia surgery at the age of 3 or at the age of 30, the result will be the same.
IF YOU DO NOT OPEN THE CANAL, YOUR CHILD WILL FAIL AT SCHOOL
WRONG ! The claim that unilateral atresia patients will fail more at school and even their earning potential will decrease is also misleading! Whether the auditory canal is opened or not, children with microtia have normal academic potential like their peers, and there are many individuals among our microtia patients who are successful in their professions such as doctors, teachers, and musicians.
IMPORTANT NOTE
ON THE OTHER HAND, All children born with bilateral microtia and atresia are recommended to use bone conduction hearing aid starting with the neonatal period in order not to delay their speaking due to lack of hearing and affect their social and academic success In later ages.
THERE WILL BE NO NEED FOR A HEARING AID AFTER CANAL SURGERY
Unfortunately It is WRONG, too !
Current clinical studies revealed that canal surgery can not provide 100% hearing even if it is performed by the most successful surgeons. Again, most of the patients will be in need to use a hearing aid.
CHILDREN CAN FIND THE DIRECTION OF THE SOUND AFTER CANAL SURGERY
WRONG ! CANAL SURGERY MAY PROVIDE SOME HEARING INCREASES BUT THE ABILITY TO FIND THE DIRECTION OF THE SOUND DOES NOT IMPROVE
Patients with unilateral atresia often complain that their voice localization is much worse than their general hearing. Therefore, there may be those who recommend surgery and canal opening. However, the results obtained from scientific clinical studies show that even in patients who may have had increased hearing after canal opening surgeries, sound localization and hearing problems experienced in noisy environments may not improve. (1,2,3,4)
In other words, after the opening of the auditory canal, the problems with finding the direction of the sound unfortunately do not improve.
IMPORTANT WARNINGS
ON THE OTHER HAND, All children born with bilateral microtia and atresia are recommended to use bone conduction hearing aid starting with the neonatal period in order not to delay their speaking due to lack of hearing and affect their social and academic success In later ages.
THE CANAL WILL NOT BE OPENED UNTIL THE CONSTRUCTION OF THE AURICLE IS COMPLETED.
The most important thing to remember about this issue is that in cases where it is decided to open the external auditory canal, the construction of the auricle must be completed before starting the opening of the canal. A doctor who suggests otherwise does not have enough information about the issue. It is very important that parents are aware of this. Because when creating a hole, the blood circulation of the skin area that will be used for the auricle is damaged and ear construction becomes difficult. In addition, the location and position of the hole to be opened is often incorrect.
In other words, unfortunately, problems with finding the direction of sound do not improve after the ear canal is opened.
DO NOT GO TOO FAR !
Another important point is that atresia surgery should be performed by an atresia surgeon located in your area. At least 20% of patients with a successful atresia procedure in the long term experience a deterioration in their results for various reasons and need a revision procedure. Even in the most experienced groups in the world, the revision rates are 15-58%! Therefore, the procedure is best performed by the surgeon who will be able to maintain the care of the new auditory canal for a long time. Unlike microtia surgery for the external ear shape, atresia surgery requires long-term care.
REFERENCES
1. Lambert PR. Congenital aural atresia: stability of surgical results. Laryngoscope. Dec 1998;108(12):1801-5.
2. De la Cruz A, Teufert KB. Congenital aural atresia surgery: long-term results. Otolaryngol Head Neck Surg. Jul 2003;129(1):121-7
3. Gray L, Kesser BW, and Cole EA. Understanding speech in noise after correction of congenital unilateral aural atresia: effects of age on the emergence of binaural squelch but not in use of head-shadow. International Journal of Pediatric Otorhinolaryngology. 2009;73:1281-7
4. Wilmington D. Gray L. Jahrsdoerfer R. Binaural processing after corrected congenital unilateral conductive hearing loss. Hearing Research. April 1994;74:99-114.